Weight Loss Surgery and Treatment
What is Obesity?
Obesity is a medical diagnosis indicating a BMI over 30. The number of affected individuals is increasing worldwide, including here in New Zealand, where we experience some of the highest rates. Obesity goes beyond skin deep; carrying excess weight has consequences for every organ in the body.
You can calculate your own BMI here:
People suffering from obesity in the modern world face numerous challenges. Society does not accommodate larger body sizes well; patients often point to airplane seats and safety belts as examples, along with difficulties in daily tasks such as tying shoelaces. To further complicate matters, easily accessible, calorie-dense fast foods are everywhere, and quality nutrition is expensive.
From a scientific perspective, we understand that people with a BMI over 35 for any length of time, often find it nearly impossible to return to a healthy weight. Currently, bariatric surgery is the only therapy known to offer these individuals long-term, sustained weight loss.
Weight Loss Medications
Weight loss medications are continuing to develop. More effective agents are being made available over time. The current generation - Saxenda, Wegovy and most recently Mounjaro (all prescription medicines) - are more effective than those available in the past. Like surgery, these medicines are tools to help manage the medical diagnosis of 'obesity', and carry risks and benefits. It is not unusual to see 10% total body weight loss with Saxenda or Wegovy. Mounjaro is further closing the gap with what surgery can offer, with early research suggesting 15% total body weight loss is achievable for many patients at standard doses (compared to 20-25% with surgery). We can't yet be clear from current evidence how reliably this weight loss persists once the medication is stopped.
These medications offer some benefit to around 80% of those who try them. Their effectiveness can wear off over time. Like surgery, they are less effectiveness in a vacuum, and work best with lifestyle change and the support of a bariatric dietitian. Mr. Stewart offers appointments to those exploring whether these medications are the right choice for them, and is happy to discuss the risks and benefits, and prescribe where appropriate. We typically commence these medications under supervision, and for those who respond well with meaningful weight loss during the first prescription, we provide advice to your GP for continuing prescriptions.
These medications are new 'tools in the toolkit' and can also play a role before or after surgery in certain individuals.
Why weight loss surgery?
Obesity has a profound impact on overall health. No organ system in the body is untouched by its effects, from the psyche to the skin, respiration to reproduction, the heart to the hips and knees. The following diagram illustrates the effects on all of the main organ systems:
Obesity is not the fault of obese people. It is a medical condition which arises from the interaction between a person’s genes and their environment. Neither is obesity simple to treat or a matter of willpower: a BMI over 35 for any length of time is very difficult to overcome without medical help for almost all sufferers. Non-surgical treatments include supervised diets, wrap-around professional support for an optimal lifestyle, weight loss medications, and endoscopic procedures such as intragastric balloons. All of these options are expensive and none of them provide the long term sustained weight loss that can be achieved with bariatric surgery.

Operations
The reason there is more than one weight loss operation is that no operation is perfect. They all induce weight loss but come with different risks and long-term issues. The choice of which one is right for you depends on your goals, stage of life, medical conditions, and risk tolerance.
All procedures are performed using laparoscopic (“keyhole”) surgery at Manuka Street Hospital, following at least two weeks of a special diet supervised by your dietitian, designed to enhance the safety of the surgery.
All commonly performed operations yield relatively similar long-term weight loss outcomes (over 3 to 20 years) and carry approximately a 10 percent risk of total weight regain.
Sleeve Gastrectomy

Roux-en-Y gastric bypass
.png?202312190402)
Sleeve Gastrectomy
This is currently the most common procedure for weight loss. It involves the permanent removal of the majority of stomach tissue, leaving behind a narrow “sleeve” of stomach. Weight loss expectations are very similar to the older gastric bypass operation but vary more between individual patients—some experience greater weight loss than others. The primary mechanism involves disrupting signals between the stomach and brain related to fullness and hunger, effectively suppressing appetite. This appetite suppression tends to diminish after one to two years. Subsequently, weight loss is maintained through continued adherence to healthy dietary habits learned in the early phases, along with the ongoing benefits of a smaller stomach. The expected total body weight loss is typically in the range of 20-30%.
The popularity of the sleeve is attributed to its shorter list of long-term side effects and lower cost due to quicker performance. Immediately after surgery, the most significant risks include bleeding or a leak from the staple line. Major bleeding affects fewer than 1 in 100 people, and a leak affects fewer than 1 in 1000. Following surgery, a 2-night hospital stay is required to ensure tolerance for adequate oral fluids and controlled pain before discharge. In the long term, the primary risk is reflux: up to 20 percent of patients may require medication to control reflux after a sleeve, and a few may request surgery to manage it. When required, this can be funded through the public sector. Lifelong vitamin supplements are recommended, but stopping them becomes less concerning after the first 2 years, provided a healthy balanced diet is maintained. For patients over 60, the sleeve is almost always recommended as it provides adequate weight loss and health improvement without excessive risk.
Roux-en-Y Gastric Bypass
This operation has been performed for many decades and has stood the test of time. Gastric bypass has a similar effect on appetite suppression as sleeve gastrectomy but also bypasses most of the stomach and the beginning of the small bowel, causing some malabsorption. Excluding this part of the gut from the food stream appears to give the bypass its ability to quite reliably switch off diabetes. If diabetes is a new diagnosis within the past 4 years, the chances of remission with a gastric bypass are 95 percent. The expected total body weight loss is 25-35%.
Bypass remains an appropriate procedure, particularly for those with diabetes and for those with severe reflux disease who would not be suitable for a sleeve. It is a longer and more complex operation to perform and carries small risks of bleeding and leaking from the joins between the stomach and small bowel. In the long term, the list of potential problems is longer: bypass patients experience “dumping” – feeling unwell from eating sugar; typically, the threshold is 10 grams or 2 teaspoons. Some people may experience dumping from lesser amounts or a wider variety of foods, and for these individuals, managing the sensation can be challenging. The join between the stomach pouch and small bowel can form a tight stricture requiring later treatment. Ulcers can form at this join, particularly if non-steroidal painkillers like Nurofen are used, or smoking is resumed. The small bowel can move through one of the gaps created by the operation, forming an “internal hernia” which requires emergency surgery to prevent life-threatening loss of the small bowel. The risk that this occurs over a lifetime can be as high as 5 percent. Finally, lifelong use of an appropriate bariatric multivitamin is critical, as well as other supplements, often B12, calcium, and iron, as deficiencies can and do occur with serious consequences.
One-anastomosis Gastric Bypass
This is a newer operation, not commonly performed internationally but gaining in popularity. It goes by various names, including 'mini-bypass.' This form of gastric bypass involves bringing a loop of the small bowel up to a long narrow stomach pouch. Consequently, it is quicker to perform than a traditional Roux-en-Y bypass but still offers many of the same benefits. While we lack long-term research on its effectiveness, it is likely to provide weight loss similar to, if not better than, a Roux-en-Y bypass. However, this comes at the expense of a higher rate of nutrient deficiencies and malnutrition, along with a heightened risk of chronic diarrhea.
Compared to Roux-en-Y gastric bypass, it carries a much lower risk of internal hernia but instead has a risk of bile reflux, which may necessitate conversion to Roux-en-Y gastric bypass for relief. Some studies report the risk of bile reflux as high as 8 percent. Based on our current understanding of this procedure, it appears to be a viable option for patients with a BMI over 50 who require significant and reliable weight loss, particularly if they are under 60 years old and have diabetes.

Revisional Surgery and Other Weight Loss Procedures
There is a wide range of other weight loss procedures, many of which are either historic and no longer performed or remain experimental. Among well-established procedures, there is a more aggressive set that causes malabsorption in addition to stomach restriction. These include the biliopancreatic diversion with duodenal switch and the single anastomosis duodenoileostomy or 'SADI,' which is a loop form of the same operation (similar to how the One-anastomosis gastric bypass is a loop form of the Roux-en-Y gastric bypass). These operations lead to profound weight loss but come at a considerable nutritional expense. SADI is recommended in certain circumstances. As it deliberately induces malabsorption, the risks include a high likelihood of nutrient deficiencies requiring correction over the long term and a relatively high rate of chronic and frequent diarrhea. It is an appropriate conversion operation for patients who have regained weight after a sleeve gastrectomy; however, these patients may also consider conversion to a One-anastomosis gastric bypass with less risk of diarrhea.
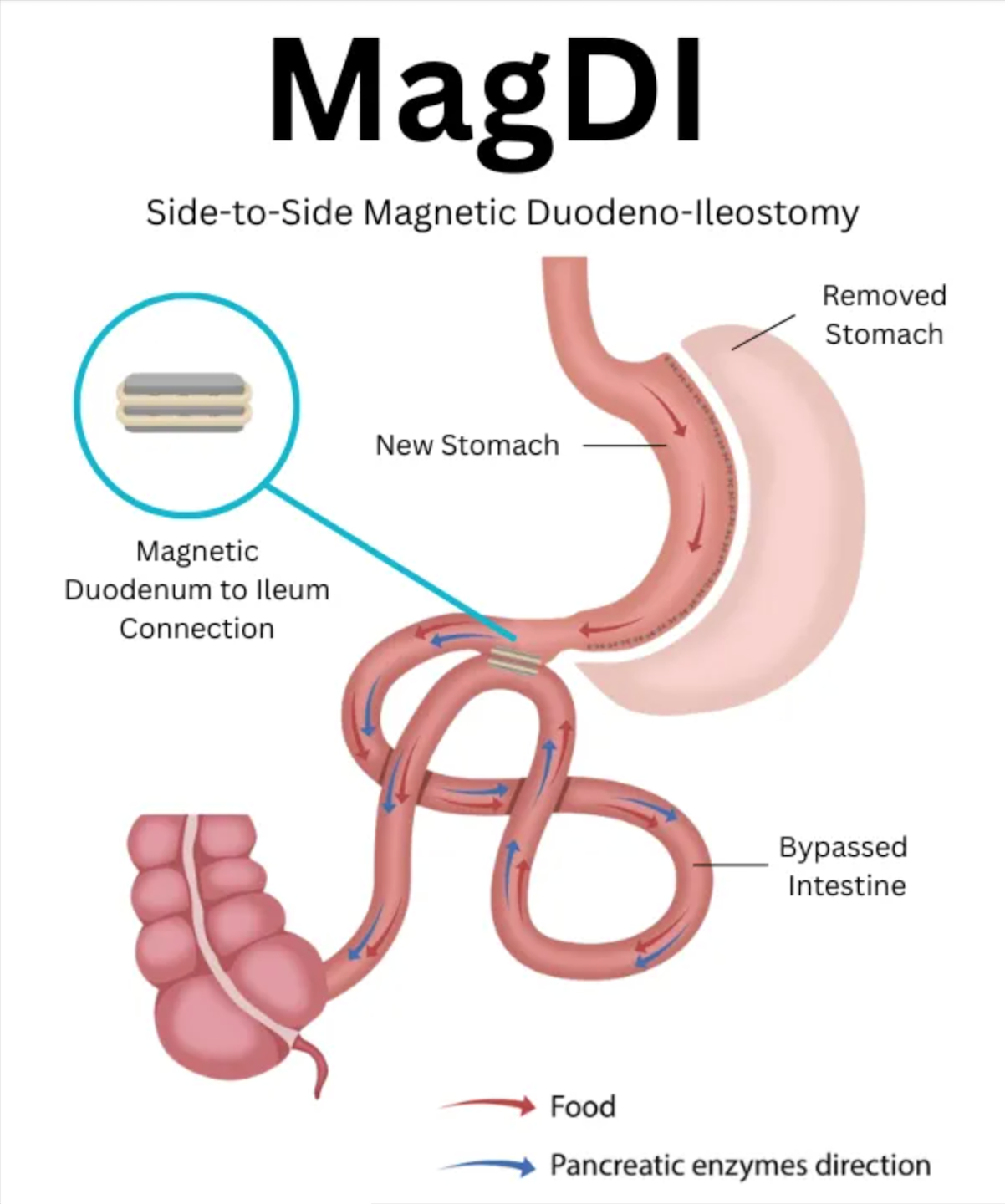
MagDI
This promising new procedure is the latest innovation in surgical weight management. It can be performed as a day stay operation. Under general anaesthetic, keyholes are made in the abdomen. Magnets placed in the duodenum and small bowel are brought together, and the operation is complete. Over several weeks, a new join opens up between the magnets, allowing the food stream to take two separate paths towards the large bowel ("double track" procedure).
This procedure can be appropriate as revision for patients with weight regain or insufficient weight loss following a sleeve gastrectomy, to improve outcomes without incurring the risk and complications of a gastric bypass. It can also be added to a sleeve at the initial surgery in patients with BMI over 50 who prefer gastric sleeve over gastric bypass, but who would benefit from more aggressive weight loss than would typically be seen with sleeve alone.
GT Metabolic is currently partnering with Nelson Weight Loss Surgery to assist New Zealand's first MagDI patients through their procedure. Please inquire with our clinic for more details.